

Jun
Wellness
When Your Palm Refuses to Unfold
If you click on links we provide, we may receive compensation.
It starts as a tiny, painless lump in the center of the palm – so small that many people dismiss it as a callus from yardwork or weightlifting. Months pass. The lump hardens, a cord rises beneath the skin, and suddenly a handshake feels awkward. For roughly five percent of adults in the United States – a figure that climbs much higher among families of Northern European descent – that quiet transformation signals the onset of Dupuytren contracture, sometimes nicknamed “Viking disease.” (verywellhealth.com, pubmed.ncbi.nlm.nih.gov) I have watched friends struggle to flatten their hands on a keyboard, unzip a jacket, or cradle a coffee cup without knocking it over. The condition can be subtle, slow, and surprisingly emotional, because the simplest gestures of daily life depend on an open palm.
A Condition with A Viking Past
Doctors first described the deformity in 1831, yet fossil evidence suggests thickened palmar fascia appeared in the hands of much earlier skeletons unearthed around the North Sea. Today the genetics remain strongest in Scandinavia, Scotland, and Ireland; studies from Norway estimate that more than one in five men over sixty show at least mild signs, though most never need surgery. (pmc.ncbi.nlm.nih.gov) Researchers link the disease to a mutation that drives fibroblasts – the ordinary cells that repair tissue – into overdrive. They churn out collagen type III in tangled bundles, and the resulting cord pulls the ring and little fingers inward. Trauma, smoking, diabetes, and heavy manual labor may accelerate the process, but heritage is usually the spark.
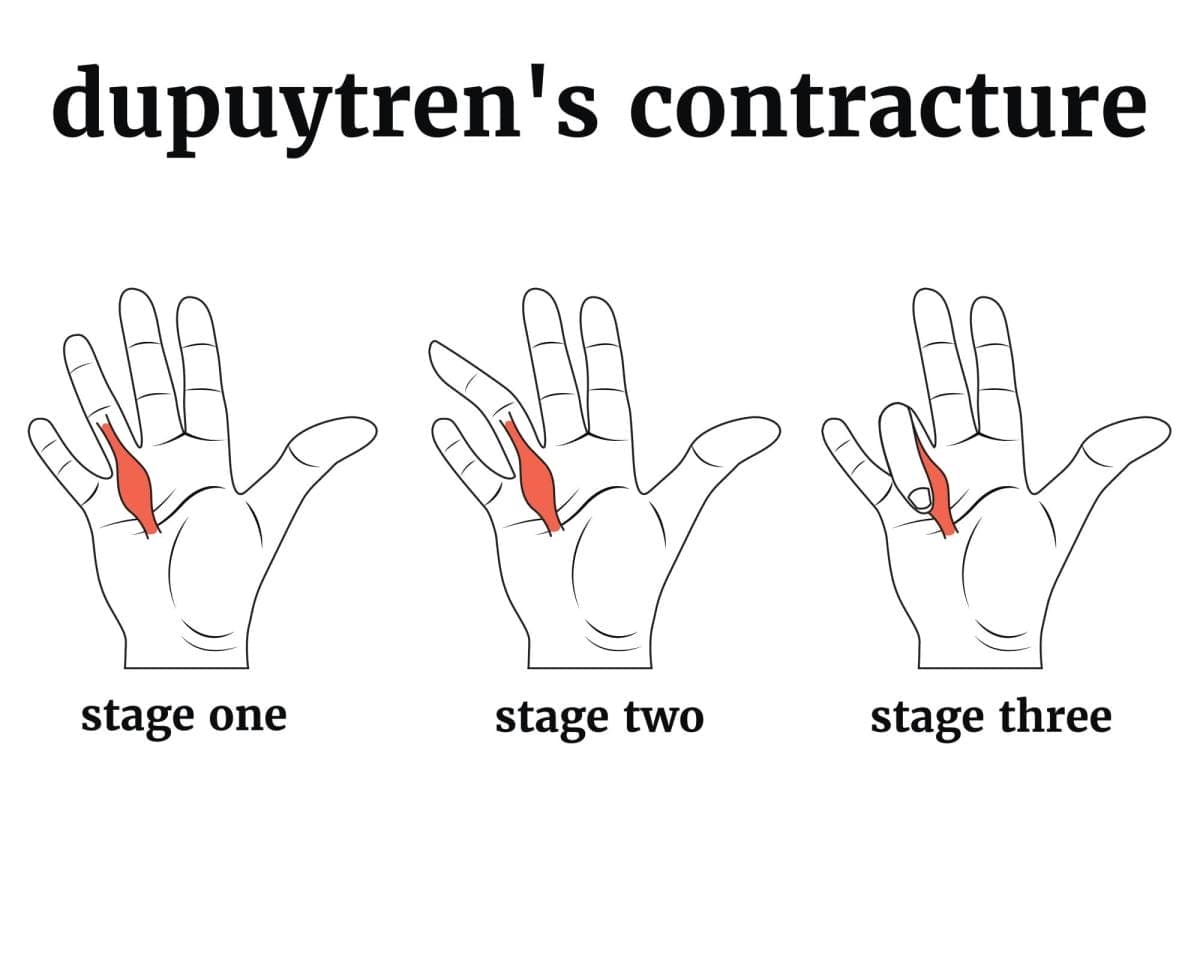
Early Nudges and Warning Signs
The first phase often feels more like a curiosity than a crisis. A soft nodule sits under the skin of the palm, tender for a week or two, then painless. Over months the nodule stiffens into a fibrous strand. At that point many notice that the palm will no longer lie flat on a tabletop. The so-called tabletop test, simple as it sounds, is the gold standard for early detection. When the cord shortens to roughly forty degrees of finger flexion, functional problems bloom: washing the face, slipping a hand into a pocket, applauding at a concert. Burning or itching accompanies the tightening in about one quarter of cases, challenging the notion that the disease is always painless. (verywellhealth.com)
Life As the Fingers Curl
Progression varies wildly. Some cords plateau for years, others climb the finger in twelve months. Because the thumb, index, and middle fingers rarely contract, people learn workarounds: typing with three fingers, opening doors with the elbow, letting voice assistants replace text messages. Still, the psychological toll is real. In surveys, nearly half of patients report embarrassment or fear of being perceived as disabled. That social component drives many to seek treatment earlier than the angles of contracture might dictate.
Why The Cord Forms – The Biology We Know
Under the microscope, Dupuytren tissue looks like a scar stuck on repeat. Mechanical stress activates myofibroblasts, which are part muscle, part fibroblast. They grip collagen and pull, exactly as they would in normal wound healing. In healthy skin, chemical signals turn that process off once a cut closes. In Dupuytren contracture, switches stay stuck in the “on” position. Scientists blame transforming growth factor-beta and Wnt pathways for the stubborn signaling, though they still cannot fully explain why the palm is the usual target. The disease can strike the soles of the feet (Ledderhose disease) or the penis (Peyronie disease), underscoring that fascia throughout the body shares the same vulnerability.
Standard Medical Options from Watchful Waiting to Knife
Doctors rank interventions by contracture angle and functional impairment. If a person can lay their hand flat and perform daily tasks, observation suffices. Corticosteroid shots can soften an early nodule but rarely change long-term destiny. Needle aponeurotomy – a twenty-minute office procedure that uses a tiny hypodermic needle to perforate the cord – releases tension immediately, yet cords return in up to sixty percent of patients within three years.
Enzyme Injections – A Decade of Data
In 2010 the U.S. Food and Drug Administration approved collagenase clostridium histolyticum, sold as Xiaflex, for adults with a palpable cord. (drugs.com) The bacterial enzyme digests peptide bonds in collagen. A day after the shot, the doctor manipulates the finger to rupture the weakened cord. Studies show roughly eighty percent of treated joints regain nearly full extension, though bruising and swelling can last weeks. Recurrence hovers around thirty to forty percent at five years – better than needle aponeurotomy, slightly worse than open surgery. (pmc.ncbi.nlm.nih.gov)
The Surgical Route and What Recovery Looks Like
For cords thicker than a pencil or joints bent beyond seventy degrees, surgeons favor limited fasciectomy: they remove the diseased fascia through zig-zag cuts that hide scars in natural creases. Recurrence can still occur, but large series report freedom from significant contracture for more than a decade in most patients. (pmc.ncbi.nlm.nih.gov) Physical therapy begins within days, focusing on edema control, scar massage, and gradual finger extension. A night splint may be worn for six months, a regimen that demands patience yet often restores the ability to place the hand flat on the table – a small victory that resonates deeply.

Exploring Natural and Conservative Care
Plenty of people hesitate at the idea of blades or enzymes. They ask about gentler avenues first, and I respect that instinct. Evidence is thinner here, but it is not absent. Therapists at OrthoBethesda outline daily stretching sequences that involve wrist extension, passive finger straightening, and gentle table push-ups. (orthobethesda.com) The goal is to maintain gliding of tendons and joints, not to rip the cord – slow, sustained tension of thirty seconds appears safest. Anecdotally, individuals who stretch during the early nodule phase report slower progression, though controlled trials are sparse.
Nutrition enters the conversation next. Curcumin, vitamin E, zinc, and magnesium earn frequent mentions in patient forums. An orthopedic team in Florida lists those supplements alongside fish oil for their anti-inflammatory and antioxidant profiles. (spineorthocenter.com) Lab studies confirm that curcumin down-regulates transforming growth factor-beta in fibroblasts, at least in petri dishes. Whether capsules translate into measurable hand improvement remains unproven, but clinicians agree they pose minimal risk when taken at recommended doses. People with clotting disorders should clear turmeric with their physician, because curcumin can thin blood.
Stretching Routines That Respect Tissue Limits
A morning ritual might unfold like this. Warm the palm in a bowl of water at about 100 °F for five minutes to soften the tissue. Lay the palm on a table. Use the other hand to press each finger knuckle toward full extension, holding for half a minute, three cycles. Follow with active gripping of a soft foam ball to keep flexor tendons from stiffening in the opposite direction. Finish with wrist circles to maintain carpal mobility. Therapists caution against quick, forceful extensions that can tear skin or cause micro-bleeds in the cord, which ironically speeds scarring.
Nutrition And Supplements – Antioxidants at Work
When patients ask me what I would take in their shoes, I mention a balanced diet first. Collagen metabolism demands vitamin C, while healthy nerve signaling that keeps the intrinsic hand muscles strong relies on B-complex vitamins. Curcumin extract of 500 mg twice daily has shown modest reductions in fibroblast proliferation in laboratory assays. Topical vitamin E oil massaged into the palm is a folk remedy with a long history but only anecdotal support; double-blind trials in scar management offer mixed results. Zinc at 15 mg daily appears safe for short courses, yet higher doses can impair copper absorption.
Heat, Massage, And Tools You Can Use at Home
Paraffin wax baths, common in arthritis clinics, deliver uniform warmth that penetrates three millimeters into tissue, enough to loosen superficial fascia. After ten minutes, many find that the palm temporarily straightens another ten degrees. A licensed massage therapist can follow with cross-fiber friction across the cord, aiming to realign collagen. Home users replicate the technique with a rubber ball pressed in slow transverse strokes. Ultrasound therapy at 1 MHz, 1.5 W/cm² for eight minutes has been studied in burn scars and may soften collagen; extrapolation to Dupuytren tissue is logical but lacks large trials.
What Science Still Needs to Prove
Randomized controlled studies of supplements, stretching, or heat remain scarce, largely because funding gravitates to patented drugs and devices. That gap breeds both optimism and misinformation. I caution patients against miracle creams or mechanical stretching gadgets advertised online. Any device that forces quick extension risks skin tears, infection, and complex regional pain syndrome. Collaborative registries now collect data on natural approaches, so we may soon know whether simple routines genuinely delay surgery.
Everyday Living Tips from Buttoning Shirts to Typing
Adaptive strategies matter. Replace small shirt buttons with magnetic closures, switch to pens with oversized grips, and raise keyboards on slanted trays so clawed fingers can strike keys from above. Speech-to-text software lightens phone use. Steering-wheel covers with thicker rims ease driving. These pragmatic edits sound mundane until you lose the ability to snap a dog leash or tap an elevator button; then they feel like liberation.
Frequently Asked Questions
Can Dupuytren contracture go away on its own?
Spontaneous reversal is exceedingly rare. Most nodules either stabilize or progress; regression tends to be partial and temporary, so monitoring remains important.
Is heavy hand use at work to blame?
Intense manual labor appears to hasten progression in people who already carry the genetic risk, but it does not cause the disease outright. Recreational grip sports tell a similar story.
Will collagenase injections weaken my tendons?
The enzyme targets collagen type I and III, abundant in cords. Flexor tendons sit deeper, shielded by synovial sheaths, and severe tendon injury is unusual when trained clinicians perform the procedure.
Do night splints really help after surgery?
Several trials show that wearing a custom thermoplastic splint for six months lowers early recurrence by about fifteen percent compared with therapy alone, though comfort and compliance vary widely.
Are herbal remedies safe with blood thinners?
Turmeric and high-dose vitamin E can increase bleeding risk. Anyone on warfarin, clopidogrel, or novel oral anticoagulants should review supplement plans with a prescribing physician before starting.
A Hand That Opens Wider Tomorrow
Dupuytren contracture reminds us that a hand is more than tendons and bones – it is a gateway to social touch and self-reliance. Modern medicine offers powerful answers, yet gentler tools like daily stretches, balanced nutrition, and mindful heat can complement the more dramatic fixes. No single path fits everyone. The goal, ultimately, is not a perfect palm but a life in which fingers once again shape clay, strum guitar strings, or simply rest flat in a friend’s grasp without pain or apology.


